0001837607
false
0001837607
2023-10-19
2023-10-19
0001837607
us-gaap:CommonStockMember
2023-10-19
2023-10-19
0001837607
us-gaap:WarrantMember
2023-10-19
2023-10-19
iso4217:USD
xbrli:shares
iso4217:USD
xbrli:shares
UNITED STATES
SECURITIES AND
EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d) of the
Securities Exchange Act of 1934
Date of Report (Date of earliest event reported):
October 19,
2023
AEON Biopharma, Inc.
(Exact name of registrant as specified in
its charter)
| Delaware |
|
001-40021 |
|
85-3940478 |
(State or other jurisdiction
of incorporation) |
|
(Commission
File Number) |
|
(IRS Employer
Identification Number) |
5
Park Plaza
Suite 1750
Irvine, CA 92614
(Address of
principal executive offices, including Zip Code)
Registrant’s telephone number, including area code: (949)
354-6499
Check the appropriate box below if the Form 8-K filing is intended
to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| |
¨ |
Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| |
¨ |
Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| |
¨ |
Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| |
¨ |
Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of
the Act:
| Title of each class |
|
Trading Symbol |
|
Name of each exchange on which registered |
| Class A Common Stock, $0.0001 par value per share |
|
AEON |
|
New
York Stock Exchange American |
| Warrants
to purchase Class A common stock |
|
AEON
WS |
|
New
York Stock Exchange American |
Indicate by check mark whether the registrant is an emerging growth
company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities
Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging growth company x
If an emerging growth company, indicate
by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial
accounting standards provided pursuant to Section 13(a) of the Exchange Act.
Item 7.01 Regulation FD Disclosure
On October 19, 2023, AEON Biopharma, Inc. (the “Company”
or “AEON”) issued a press release announcing certain clinical updates, a copy of which is furnished as Exhibit 99.1 to this
Form 8-K and incorporated herein by reference.
On October 19, 2023, the Company made available in the investor
relations section of its website a presentation relating to such clinical updates, a copy of which is furnished as Exhibit 99.2 to
this Form 8-K and incorporated herein by reference. Also on October 19, 2023, the Company made available in the investor relations section of its website a presentation, a copy of which
is furnished as Exhibit 99.3 to this Form 8-K and incorporated herein by reference.
The information furnished under this Item 7.01 (including Exhibits
99.1, 99.2 and 99.3) shall not be deemed “filed” for purposes of Section 18 of the Exchange Act or otherwise subject to the liabilities
of that section, nor shall it be deemed to be incorporated by reference into any filing of the Company under the Securities Act or the
Exchange Act, except as expressly set forth by specific reference in such a filing.
Item 8.01 Other Events
Clinical Updates
On October 19, 2023, the Company announced results for its
Phase 2 randomized, double-blind, placebo-controlled study evaluating the efficacy and safety of ABP-450 for the prevention of
episodic migraine in adults. The Company projects that approximately 9.4 million Americans live with episodic migraine, which is
characterized by fewer than 15 headache days per month and between 6 to 14 migraine days per month, but each individual attack can
be just as debilitating.
The Phase 2 study enrolled a total of 305 patients across approximately
60 sites in the United States, Canada and Australia. Patients had at least a one-year history of episodic migraine (with or without aura)
according to the ICHD-3 (2018) definition and diagnostic criteria. Patients were randomized approximately evenly across a low dose group
receiving 150 units (150U) of ABP-450, a high dose group receiving 195 units (195U) of ABP-450, and a placebo group. All patients received
two treatment cycles 12 weeks apart utilizing the Company’s novel treatment paradigm involving fewer injections than the current
botulinum toxin treatment option for chronic migraine.
The primary endpoints for the clinical study were the change in mean
monthly migraine days, or MMD, from the four-week baseline period to weeks 21 to 24 of the treatment period and the incidence of treatment-emergent
adverse events (“TEAEs”), in each case as compared to placebo. The key secondary and exploratory endpoints included the percentage
of patients achieving a reduction from baseline (the “responder rate”) of at least 50% in MMD and 75% in MMD during the weeks
21 to 24 of the treatment period and improvements on certain patient and rating scales.
On the primary endpoint, the topline data showed ABP-450 had a robust
treatment effect with mean reductions in MMD of 4.8 days (150U dose, n = 99) and 5.0 days (195U dose, n = 108), which is numerically superior
to 4.2 days (placebo, n = 98) at weeks 21-24 but did not meet statistical significance. On the key secondary endpoint of MMD responder
rates, ABP-450 did show statistical significance and clinically meaningful separation from placebo. Sixty-nine percent of patients at
195U dose achieved a 50% or greater reduction in MMD, which was statistically superior to placebo at 52% (p=0.0132). Thirty-seven percent
of patients receiving the 195U dose and 34% of patients receiving the 150U dose achieved 75% or greater reduction in MMD, which were both
statistically superior to placebo at 23% (p=0.0245 and p=0.0439, respectively). On the exploratory endpoint of Patient Global Impression
of Severity (PGI-S), the results showed statistically superior improvements of -0.9 (150U dose) and -1.0 (195U dose) compared to placebo
at -0.6 (p=0.0436 and p=0.0028, respectively).
ABP-450 demonstrated a favorable safety profile for patients with episodic
migraine. The Company believes the totality of the data provides evidence of a dose response favoring the higher 195U dose and lends support
to its decision to progress ABP-450 into Phase 3. The Company plans to request an end-of-phase 2 meeting with the U.S. Food and Drug Administration
(FDA) to discuss the protocol and study design for Phase 3, and the meeting is expected to take place in the first half of 2024.
Cautionary Note Regarding Forward-Looking Statements
Certain statements in this Form 8-K may be considered
forward-looking statements. Forward-looking statements generally relate to future events or AEON’s future financial or
operating performance. For example, statements regarding continued listing on the New York Stock Exchange American, the anticipated
timing of clinical results, the impact of current financing arrangements, the competitive environment in which AEON operates,
AEON’s expected capital resources and liquidity needs and the expected future operating and financial performance and market
opportunities of AEON are forward-looking statements. In some cases, you can
identify forward-looking statements by terminology such as "pro forma", "may", "should", "could",
"might", "plan", "possible", "project", "strive", "budget", "forecast",
"expect", "intend", "will", "estimate", "anticipate", "believe", "predict",
"potential" or "continue", or the negatives of these terms or variations of them or similar terminology. Such
forward-looking statements are subject to risks, uncertainties, and other factors which could cause actual results to differ
materially from those expressed or implied by such forward-looking statements.
These forward-looking statements are based upon estimates and
assumptions that, while considered reasonable by AEON and its management, are inherently uncertain. Factors that may cause actual
results to differ materially from current expectations include, but are not limited to: (i) the outcome of any legal proceedings
that may be instituted against AEON or others; (ii) AEON’s ability to continue to meet continued stock exchange listing
standards; (iii) costs related to being a public company; (iv) changes in applicable laws or regulations; (v) the possibility that
AEON may be adversely affected by other economic, business, regulatory, and/or competitive factors; (vi) AEON’s estimates of
expenses and profitability; (vii) the evolution of the markets in which AEON competes; (viii) the ability of AEON to implement its
strategic initiatives, including the continued development of ABP-450; (ix) the ability of AEON to defend its intellectual property;
(x) the ability of AEON to satisfy regulatory requirements; (xi) the impact of adverse geopolitical and macroeconomic developments,
such as the COVID-19 pandemic, the Israel-Hamas conflict, the Ukraine-Russia conflict and related sanctions, actual and
anticipated changes in interest rates, economic inflation and the responses by central banking authorities to control such
inflation, on AEON’s business; and (xii) other risks and uncertainties set forth in the sections entitled “Risk
Factors” and “Cautionary Note Regarding Forward-Looking Statements” in the Company’s prospectus and in
subsequent filings with the Securities and Exchange Commission.
Nothing in this Form 8-K should be regarded as a representation
by any person that the forward-looking statements set forth herein will be achieved or that any of the contemplated results of such
forward-looking statements will be achieved. You should not place undue reliance on forward-looking statements, which speak only as
of the date they are made. AEON does not undertake any duty to update these forward-looking statements.
Item 9.01 Financial Statements and Exhibits
(d) Exhibits.
SIGNATURES
Pursuant to the requirements of the Securities
Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| |
AEON
Biopharma, Inc. |
| |
|
|
| Date: October 19, 2023 |
By: |
/s/ Marc Forth |
| |
|
Marc Forth |
| |
|
Chief Executive Officer |
Exhibit 99.1
 |
PRESS RELEASE |
AEON Biopharma
Announces Topline Results from Phase 2 Trial of ABP-450
(prabotulinumtoxinA) for the Preventive Treatment of Episodic Migraine
– ABP-450
doses of 150 units and 195 units showed treatment effect of 4.8 days and 5.0 days, respectively, in the mean change from baseline in
monthly migraine days (MMD) at weeks 21-24 but did not meet statistical significance vs. placebo because of a much higher-than-expected
placebo response of 4.2 days –
– Study
demonstrated statistical significance on multiple secondary and exploratory endpoints, including the responder analysis of both a >50%
and >75% improvement from baseline in MMD –
– Totality
of the data showed evidence of a dose response favoring the higher 195 units arm, and supports the decision to advance into Phase 3,
anticipated in 2H 2024 –
– Ongoing
Phase 2 trial for the preventive treatment of chronic migraine has enrolled over 430 subjects; anticipate completing enrollment in Q4
2023 and announcing topline data in 2H 2024 –
– Management
to host a conference call at 4:30 p.m. ET –
IRVINE, Calif.,
October 19, 2023 – AEON Biopharma, Inc. (“AEON” or the “Company”) (NYSE: AEON, AEON WS), a clinical-stage
biopharmaceutical company focused on developing a proprietary botulinum toxin complex for the treatment of multiple debilitating medical
conditions, announced the topline results from its Phase 2 clinical trial of ABP-450 (prabotulinumtoxinA) for the preventive treatment
of episodic migraine.
The Phase 2 randomized,
double-blind, placebo-controlled trial evaluated the efficacy and safety of ABP-450 for the prevention of episodic migraine in adults
who suffer from fewer than 15 headache days per month and between 6 to 14 migraine days per month. The study enrolled a total of 305
patients across approximately 60 sites in the United States, Canada and Australia. Patients had at least a one-year history of episodic
migraine (with or without aura) according to the ICHD-3 (2018) definition and diagnostic criteria. Patients were randomized approximately
evenly across a low dose group receiving 150 units (150U) of ABP-450, a high dose group receiving 195 units (195U) of ABP-450, and a
placebo group. All patients received two treatment cycles 12 weeks apart utilizing the Company’s novel treatment paradigm involving
fewer injections than the current botulinum toxin treatment option for chronic migraine.
The primary endpoints for the clinical
study were the change in mean monthly migraine days, or MMD, from the four-week baseline period to weeks 21 to 24 of the treatment period
and the incidence of treatment-emergent adverse events (“TEAEs”), in each case as compared to placebo. The key secondary
and exploratory endpoints included the percentage of patients achieving a reduction from baseline (the “responder rate”)
of at least 50% in MMD and 75% in MMD during the weeks 21 to 24 of the treatment period and improvements on certain patient and rating
scales.
On the primary
endpoint, the topline data showed ABP-450 had a treatment effect with mean reductions in MMD of 4.8 days at the 150U dose (n = 99) and
5.0 days at the 195U dose (n = 108), compared to only 4.2 days in placebo (n = 98) at weeks 21-24, but did not meet statistical significance
(Figure 1). On the key secondary endpoint of MMD responder rates, ABP-450 did show statistical significance and clinically meaningful
separation from placebo. Sixty-nine percent of patients at the 195U dose achieved a 50% or greater reduction in MMD, which was statistically
significant to placebo at 52% (p=0.0132). Thirty-seven percent of patients receiving the 195U dose and 34% of patients receiving the
150U dose achieved 75% or greater reduction in MMD, which were both statistically significant to placebo at 23% (p=0.0245 and p=0.0439,
respectively). Results of the responder rate analysis are summarized in Figure 2. On the exploratory endpoint of Patient Global Impression
of Severity (PGI-S), the results showed statistically significant improvements of -0.9 at the 150U dose and -1.0 at the 195U dose, compared
to placebo at -0.6 (p=0.0436 and p=0.0028, respectively).
| |
PRESS RELEASE |
ABP-450 demonstrated
a favorable safety profile for patients with episodic migraine. The Company believes the totality of the data provides evidence of a
dose response favoring the higher 195U dose and lends support to its decision to progress ABP-450 into Phase 3. The Company plans to
request an end-of-phase 2 meeting with the U.S. Food and Drug Administration (FDA) to discuss the protocol and study design for Phase
3, and the meeting is expected to take place in the first half of 2024.
“These Phase
2 results offer encouraging data around reductions in MMD, dose response, and safety and tolerability that warrant progressing into Phase
3 with ABP-450 for the preventive treatment of episodic migraine. We believe that the inclusion of a high percentage of naïve patients
within the study may have contributed to a higher than expected response rate among patients receiving placebo. For Phase 3, we are evaluating
multiple parameters to increase the statistical power and reduce the observed higher placebo responses,” stated Dr. Chad Oh, Chief
Medical Officer of AEON.
“We believe
these robust topline data announced today from the Phase 2 trial fulfill our objectives for this study and support the decision to advance
the program into a larger pivotal study. We look forward to meeting with the FDA during an end-of-phase 2 meeting to solidify our Phase
3 program,” commented Marc Forth, AEON’s President and Chief Executive Officer. “In addition, we are on track to complete
enrollment in our ongoing Phase 2 study of ABP-450 as a preventive treatment for chronic migraine in the fourth quarter of 2023 and announce
the topline data in the second half of 2024.”
Figure 1
- Change in Monthly Migraine Days (MMD) (Weeks 21-24)

Caption: p=0.2844
(150 U vs. Placebo); and p=0.1711 (195 U vs. Placebo)
| |
PRESS RELEASE |
Figure 2
- MMD Responder Rates Statistically Significant

Caption: Responder
definition: patient demonstrated a reduction vs. baseline in the number of monthly migraine days (MMD) of ≥50% and ≥75% during
weeks 21-24
Migraine is a complex
neurological disease characterized by recurrent episodes of headaches that affects approximately 40 million people in the United States
and approximately a billion people worldwide, making migraine the third most prevalent illness in the world. Patients that live with
migraine experience symptoms that include recurring throbbing headache pain, nausea, vomiting, and sensitivity to light, sound, touch
and smell. Migraine can be categorized as episodic migraine or chronic migraine. The Company projects that approximately 9.4 million
Americans live with episodic migraine, which is characterized by fewer than 15 headache days per month and between 6 to 14 migraine days
per month, but each individual attack can be just as debilitating.
Conference Call and Webcast Information
AEON will host
an analyst and investor conference call at 4:30 p.m. ET today, October 19, 2023, which will include a more detailed presentation of these
data. To access the webcast of the call with slides please visit the Investors section of AEON’s website or Click Here for
a direct link. An archived webcast will be available on the AEON website after the event. For those wishing to access the conference
call via phone, please dial +1 (877) 704-4453 (domestic) or +1 (201) 389-0920 (international).
To learn more about
AEON and the development of its uniquely positioned therapeutic neurotoxin, visit www.aeonbiopharma.com.
| |
PRESS RELEASE |
About ABP-450
(prabotulinumtoxinA) Injection
ABP-450 contains
a 900 kDa botulinum toxin type-A complex produced by the bacterium Clostridium botulinum. The active part of the botulinum toxin is the
150 kDa component, and the remaining 750 kDa of the complex is made up of accessory proteins that the Company believes help with the
function of the active portion of the botulinum toxin. When injected at therapeutic levels, ABP-450 blocks peripheral acetylcholine release
at presynaptic cholinergic nerve terminals by cleaving SNAP-25, a protein integral to the successful docking and release of acetylcholine
from vesicles situated within the nerve endings leading to denervation and relaxation of the muscle.
About AEON Biopharma
AEON is a clinical
stage biopharmaceutical company focused on developing its proprietary botulinum toxin complex, ABP-450 (prabotulinumtoxinA) injection,
or ABP-450, for debilitating medical conditions, with an initial focus on the neurosciences market. AEON recently completed a Phase 2
study of ABP-450 for the treatment of cervical dystonia and has an ongoing Phase 2 study of ABP-450 for the preventive treatment of chronic
migraine. ABP-450 is the same botulinum toxin complex that is currently approved and marketed for cosmetic indications by Evolus under
the name Jeuveau. ABP-450 is manufactured by Daewoong in compliance with current Good Manufacturing Practice, or cGMP, in a facility
that has been approved by the U.S. Food and Drug Administration, or the FDA, Health Canada and European Medicines Agency, or EMA. AEON
has exclusive development and distribution rights for therapeutic indications of ABP-450 in the United States, Canada, the European Union,
the United Kingdom, and certain other international territories. The Company has built a highly experienced management team with specific
experience in biopharmaceutical and botulinum toxin development and commercialization.
Forward-Looking
Statements
Certain statements
in this press release may be considered forward-looking statements. Forward-looking statements generally relate to future events or AEON’s
future financial or operating performance. For example, statements regarding continued listing on the New York Stock Exchange American,
the anticipated timing of clinical results, the impact of current financing arrangements, the competitive environment in which AEON operates,
AEON’s expected capital resources and liquidity needs and the expected future operating and financial performance and market opportunities
of AEON are forward-looking statements. In some cases, you can identify forward-looking statements by terminology such as "pro forma",
"may", "should", "could", "might", "plan", "possible", "project",
"strive", "budget", "forecast", "expect", "intend", "will", "estimate",
"anticipate", "believe", "predict", "potential" or "continue", or the negatives of
these terms or variations of them or similar terminology. Such forward-looking statements are subject to risks, uncertainties, and other
factors which could cause actual results to differ materially from those expressed or implied by such forward-looking statements.
| |
PRESS RELEASE |
These forward-looking
statements are based upon estimates and assumptions that, while considered reasonable by AEON and its management, are inherently uncertain.
Factors that may cause actual results to differ materially from current expectations include, but are not limited to: (i) the outcome
of any legal proceedings that may be instituted against AEON or others; (ii) AEON’s ability to continue to meet continued stock
exchange listing standards; (iii) costs related to being a public company; (iv) changes in applicable laws or regulations; (v) the possibility
that AEON may be adversely affected by other economic, business, regulatory, and/or competitive factors; (vi) AEON’s estimates
of expenses and profitability; (vii) the evolution of the markets in which AEON competes; (viii) the ability of AEON to implement its
strategic initiatives, including the continued development of ABP-450; (ix) the ability of AEON to defend its intellectual property;
(x) the ability of AEON to satisfy regulatory requirements; (xi) the impact of adverse geopolitical and macroeconomic developments, such
as the COVID-19 pandemic, the Israel-Hamas conflict, the Ukraine-Russia conflict and related sanctions, actual and anticipated changes
in interest rates, economic inflation and the responses by central banking authorities to control such inflation on AEON’s business;
and (xii) other risks and uncertainties set forth in the section entitled “Risk Factors” and “Cautionary Note Regarding
Forward-Looking Statements” in the Company’s prospectus and in subsequent filings with the Securities and Exchange Commission.
Nothing in this
press release should be regarded as a representation by any person that the forward-looking statements set forth herein will be achieved
or that any of the contemplated results of such forward-looking statements will be achieved. You should not place undue reliance on forward-looking
statements, which speak only as of the date they are made. AEON does not undertake any duty to update these forward-looking statements.
Contacts
Investor Contact:
Corey Davis, Ph.D.
LifeSci Advisors
+1 212 915 2577
cdavis@lifesciadvisors.com
Source: AEON Biopharma
Exhibit 99.2

Phase 2 Topline Results Preventive Treatment of Episodic Migraine October 2023 ABP - 450 ( prabotulinumtoxinA)

2 Forward Looking Statements Certain statements in this presentations may be considered forward - looking statements . Forward - looking statements generally relate to future events or AEON’s future financial or operating performance . For example, statements regarding continued listing on the New York Stock Exchange American, the anticipated timing of clinical results, the impact of current financing arrangements, the competitive environment in which AEON operates, AEON’s expected capital resources and liquidity needs and the expected future operating and financial performance and market opportunities of AEON are forward - looking statements . In some cases, you can identify forward - looking statements by terminology such as "pro forma", "may", "should", "could", "might", "plan", "possible", "project", "strive", "budget", "forecast", "expect", "intend", "will", "estimate", "anticipate", "believe", "predict", "potential" or "continue", or the negatives of these terms or variations of them or similar terminology . Such forward - looking statements are subject to risks, uncertainties, and other factors which could cause actual results to differ materially from those expressed or implied by such forward - looking statements . These forward - looking statements are based upon estimates and assumptions that, while considered reasonable by AEON and its management, are inherently uncertain . Factors that may cause actual results to differ materially from current expectations include, but are not limited to : (i) the outcome of any legal proceedings that may be instituted against AEON or others ; (ii) AEON’s ability to continue to meet continued stock exchange listing standards ; (iii) costs related to being a public company ; (iv) changes in applicable laws or regulations ; (v) the possibility that AEON may be adversely affected by other economic, business, regulatory, and/or competitive factors ; (vi) AEON’s estimates of expenses and profitability ; (vii) the evolution of the markets in which AEON competes ; (viii) the ability of AEON to implement its strategic initiatives, including the continued development of ABP - 450 ; (ix) the ability of AEON to defend its intellectual property ; (x) the ability of AEON to satisfy regulatory requirements ; (xi) the impact of adverse geopolitical and macroeconomic developments, such as the COVID - 19 pandemic, the Israel - Hamas conflict, the Ukraine - Russia conflict and related sanctions, actual and anticipated changes in interest rates, economic inflation and the responses by central banking authorities to control such inflation on AEON’s business ; and (xii) other risks and uncertainties set forth in the section entitled “Risk Factors” and “Cautionary Note Regarding Forward - Looking Statements” in the Company’s prospectus and in subsequent filings with the Securities and Exchange Commission . Nothing in this presentation should be regarded as a representation by any person that the forward - looking statements set forth herein will be achieved or that any of the contemplated results of such forward - looking statements will be achieved . You should not place undue reliance on forward - looking statements, which speak only as of the date they are made . AEON does not undertake any duty to update these forward - looking statements

3 Primary Endpoint Mean reduction in monthly migraine days (MMD) of 4.8 days ( 150U) and 5.0 days (195U) was numerically superior to placebo (4.2 days) at weeks 21 - 24, but did not meet statistical significance Phase 2 Data in Episodic Migraine Provides Confidence to Move to Phase 3 Key Secondary Endpoint and Exploratory Endpoint hit statistical significance 69% of patients receiving the 195U dose achieved a 50% or greater reduction in MMDs, which was statistically significant to placebo at 52% (p=0.0132); 37% of patients receiving the 150U dose and 34% of patients receiving the 195 U dose achieved a 75% or greater reduction in MMDs , which was statistically significant to placebo at 23% (p=0.0245, p=0.0439, respectively) Patient global assessment – statistically significant for both 150U (p=0.0436) and 195U (p=0.0028) x Observations Change in MMD over time shows: 1) evidence of a dose response in favor of 195U and 2) durability of response over weeks 13 - 24 (after administration of the 2 nd dose cycle) N umerical reduction of 4.8 - 5.0 MMDs is higher than all Phase 3 CGRP studies H igh placebo response (4.2 MMDs) possibly due to inclusion of high number of naïve patients x x x x

4 Addressable Patient Population ~3x Higher with Episodic Indication 1. Prevention of chronic migraine is currently approved indication for Botox 2. No botulinum toxin is approved for prevention of episodic migraine 1.6M Total Addressable Patients 260M People 2020 US 18+ Population 40M Patients (15%) Estimated Migraine and severe HA Patients 9.4M Patients (24%) Episodic Migraine (<15 HA days and 6 - 14 M days month) 4.0M Patients (10%) Chronic Migraine (15+ HA days and 8+ M days /month) 2.2M Patients (56%) Diagnosed Prevalence 3.7M Patients (39%) Diagnosed Prevalence 820k Patients (37%) Treated Patients (Prophylactic) 740k Patients (20%) Treated Patients (Prophylactic) Chronic Migraine 1 Episodic Migraine 2

5 Overview of Phase 2 Study in Episodic and Chronic Migraine 1 Dodick , et. al.; OnabotulinumtoxinA for Treatment of Chronic Migraine; Headache (2010); volume 50(6):919 - 1102 • N = 765 • ~60 sites in US, Canada & Australia • Includes both EM & CM patients • # headache days and migraine days/month established during 4 - week baseline prior to randomization • 3 arms: 150 Units, 195 Units, PBO • 2 injection cycles, 3 months apart • 6 - month treatment duration • Novel injection paradigm: - 22 injection sites (ABP - 450 low dose) - vs. 31 injections for Botox 1 Primary: • Mean change of monthly migraine days (MMD) on weeks 21 - 24 • Incidence of TEAEs throughout study compared to placebo Secondary: • Percentage of patients with reduction from baseline of ≥50%, 75%, 100% in mean number of MMD throughout the study • Mean change of monthly headache days (MHD) on weeks 21 - 24 • Change in use of rescue medications from baseline Exploratory: • Change in PGI - S, PGI - C, MIDAS, etc. Placebo n= 255 195 Units ABP - 450 n= 255 24 weeks Primary Efficacy Endpoint 150 Units ABP - 450 n= 255 4 - week Baseline 4 - week Screening Randomized R Endpoints Randomized Double - Blinded Placebo - Controlled Study Open Label Extension Study 4 treatments of ABP - 450 52 weeks Study Design 12 weeks Objective: To evaluate the efficacy and safety of ABP - 450 in EM and CM

6 Phase 2 Program Stratified for Episodic and Chronic Migraine Headache Day is defined as: Migraine Day or Non - Migraine Headache Day Migraine Day is defined as: • At least 4 continuous hours of headache over the course of 1 Calendar Day per ICHD - 3 Criteria: o Migraine without aura o Migraine with aura o Probable migraine (protocol specific, as there is no 4 - hour requirement per ICHD - 3 Criteria) • Treatment - aborted migraine per ICHD - 3 Criteria (<4 hours in duration) Non - Migraine Headache Day is defined as: • At least 4 continuous hours of headache of at least moderate intensity over the course of 1 Calendar Day and does not meet criteria for a migraine day, or a day with a headache that is successfully treated with an acute medication not specific to migraine. Episodic Migraine N=305 <15 headache days / month And 6 - 14 migraine days / month 150 U N=99 195 U N=108 Placebo N=98 Final Analysis of the Episodic Cohort Fall 2023 Chronic Migraine N=~465 ≥ 15 headache days / month And ≥ 8 migraine days / month 150 U N=155 195 U N=155 Placebo N=155 Final Analysis of the Chronic Cohort Anticipated 2024 Randomization and Stratified for Episodic Migraine and Chronic Migraine

7 Phase 2 Episodic Migraine: Subject Disposition Disposition Analysis Placebo n (%) ABP - 450 150 units n (%) ABP - 450 195 units n (%) Total n (%) Randomized 98 99 108 305 Safety Analysis Set 97 (99.0) 99 (100) 109 (101) 305 (100) Full Analysis Set ( Fas *) 98 (100) 99 (100) 108 (100) 305 (100) Study Completed 86 (87.8) 84 (84.8) 90 (83.3) 260 (85.2) Study Discontinued 12 (12.2) 15 (15.2) 18 (16.7) 45 (14.8) Modified Full Analysis Set ( mFAS *) 90 (91.8) 92 (92.9) 96 (88.9) 278 (91.1) Per Protocol Analysis Set (PP) 82 (83.7) 83 (83.8) 86 (79.6) 251 (82.3) Primary Reasons For Study Discontinuation Adverse Event 0 1 (1.0) 3 (2.8) 4 (1.3) Withdrew Consent 7 (7.1) 6 ( 6.1) 11 (10.2) 24 (7.9) Lost To Follow - up 5 (5.1) 7 (7.1) 4 (3.7) 16 (5.2) Other 0 1 (1.0) 0 1 (0.3) * FAS is the same as intent to treat population (ITT) and mFAS is the same as modified ITT ( mITT ) mFAS – patients have received at least 2 doses of study medication Prespecified statistical analysis used mFAS for all primary and key secondary efficacy endpoint assessments

8 Demographics and Baseline Characteristics Headache Day is defined as: Migraine Day or Non - Migraine Headache Day Migraine Day is defined as: • At least 4 continuous hours of headache over the course of 1 Calendar Day per ICHD - 3 Criteria: o Migraine without aura o Migraine with aura o Probable migraine (protocol specific, as there is no 4 - hour requirement per ICHD - 3 Criteria) • Treatment - aborted migraine per ICHD - 3 Criteria (<4 hours in duration) Non - Migraine Headache Day is defined as: • At least 4 continuous hours of headache of at least moderate intensity over the course of 1 Calendar Day and does not meet criteria for a migraine day, or a day with a headache that is successfully treated with an acute medication not specific to migraine. Parameter Placebo (N=90) ABP - 450 150 units (N=92) ABP - 450 195 units (N=96) Total (N=278) Mean Age (SD) 47.0 (12.43) 45.0 (11.52) 44.9 (11.75) 45.6 (11.90) Female (%) 76 (84.4) 74 (80.4) 81 (84.4) 231 (83.1) Race, n (%) White 80 (88.9) 76 (82.6) 82 (85.4) 238 (85.6) Black or African American 7 (7.8) 12 (13.0) 11 (11.5) 30 (10.8) Asian 3 (3.3) 0 2 (2.1) 5 (1.8) Other 0 4 (4.3) 1 (1.0) 5 (1.8) MEAN BMI (kg/m 2 ) (SD) 28.49 (5.369) 28.04 (4.393) 28.58 (4.960) 28.37 (4.909) Number 0f Headache Days at Baseline 10.7 (2.07) 10.8 (2.21) 10.2 (2.13) 10.6 (2.15) Number of Migraine Days at Baseline 9.4 (2.19) 9.9 (2.30) 8.9 (2.02) 9.4 (2.20)

9 Primary Endpoint: Change in Monthly Migraine Days (MMD) (Weeks 21 - 24) 1 See slide 16 - 4.2 (44.7%) - 4.8 (48.5%) - 5.0 (56.2%) - 0.6 - 0.8 -6 -5 -4 -3 -2 -1 0 Placebo (n=90) 150 U (n=92) 195 U (n=96) Mean Change From Baseline MMD LS Mean Diff (vs. Pl) p = 0. 2844 ( 150 U vs. Placebo) p=0. 1711 ( 195 U vs. Placebo ) • N umerical reduction of 4.8 - 5.0 migraine days is higher than the active arm in all Phase 3 CGRP studies 1

10 Secondary Endpoint: MMD Responder Rates Statistically Significant * Statistically significant 52.1 58.9 69.0 0 10 20 30 40 50 60 70 80 Placebo (n=90) 150 U (n=92) 195 U (n=96) Rate (%) p=0. 2459 (150 U vs. p lacebo) p=0. 0132 (195 U vs. p lacebo) 22.5 37.0 33.8 0 10 20 30 40 50 60 70 80 Placebo (n=90) 150 U (n=92) 195 U (n=96) Rate (%) p=0. 0245 (150 U vs. p lacebo) p=0. 0439 (195 U vs. p lacebo) R esponder definition: patient demonstrated a reduction vs. baseline in the number of monthly migraine days (MMD) of ≥ 50% and ≥ 75% during weeks 21 - 24 * * * Responder Rate (≥75% reduction in MMDs ) Responder Rate (≥50% reduction in MMDs )

11 Secondary Endpoint: Change in Monthly Headache Days (MHD) (Weeks 21 - 24) - 4.7 (43.9%) - 5.1 (47.2%) - 5.7 (55.8%) - 0.4 - 1 .0 -6 -5 -4 -3 -2 -1 0 Placebo (n=90) 150 U (n=92) 195 U (n=96) Mean Change From Baseline MHD LS Mean Diff (vs. Pl) p = 0. 5118 ( 150 U vs. Placebo) p=0. 1182 ( 195 U vs. Placebo)

12 Change in Migraine Days (MMD) Over Time Shows Evidence of Dose Response 2 nd dose cycle administered at week 12 -6.0 -5.0 -4.0 -3.0 -2.0 -1.0 0.0 0 4 8 12 16 20 24 Placebo 195 U P=0.1315 P=0.1496 -6.0 -5.0 -4.0 -3.0 -2.0 -1.0 0.0 0 4 8 12 16 20 24 Placebo 150 U p=0.0602 p=0.3037 • Lower 150U dose shows waning efficacy towards end of dosing interval • Period from 17 - 24 weeks demonstrates highest degree of separation

13 Change in Headache Days (MHD) Over Time Shows Evidence of Dose Response -7.0 -6.0 -5.0 -4.0 -3.0 -2.0 -1.0 0.0 0 4 8 12 16 20 24 Placebo 195 U P=0.1182 P=0.0513 -7.0 -6.0 -5.0 -4.0 -3.0 -2.0 -1.0 0.0 0 4 8 12 16 20 24 Placebo 150 U p=0.0740 p=0.5118 2 nd dose cycle administered at week 12

14 MMD Responder Rates Over Time Show Evidence of Dose Response Responder Rate (≥50%) Responder Rate (≥75%) • From 5 - weeks onward, >30% patients on 195U demonstrated > 75% reduction in monthly migraine days

15 Exploratory Endpoint: Patient Global Impression of Severity (PGI - S) was Statistically Significant * Statistically significant - 0.6 - 0.9 - 1 - 0.3 - 0.4 -1.2 -1 -0.8 -0.6 -0.4 -0.2 0 Placebo (n=90) 150 U (n=92) 195 U (n=96) Mean PGI - S LS Mean Diff (vs. Pl) p = 0. 0436 ( 150 U vs. p lacebo) p=0. 0028 ( 195 U vs. p lacebo) * *

16 Brand Generic Trial Duration Dose Primary endpoint N Change (days) Diff. from PBO p - value Aimovig erenumab STRIVE 24 wks 70 mg SC QM MMD (change from baseline to months 4 - 6) 312 - 3.2 - 1.4 <0.001 140 mg SC QM 318 - 3.7 - 1.9 <0.001 Placebo 316 - 1.8 — — ARISE 12 wks 70 mg SC QM MMD (change from baseline in last 4 wks of trial) 282 - 2.9 - 1.1 <0.001 Placebo 288 - 1.8 — — Ajovy fremanezumab 12 wks 225 mg SC QM MMD (change during 12wk trial, after 1st dose) 287 - 3.7 - 1.5 <0.001 675 mg SC Q3M 288 - 3.4 - 1.2 <0.001 Placebo 290 - 2.2 — — Emgality galcanezumab EVOLVE - 1 6 months 120 mg SC QM MMD (change from baseline during treatment) 210 - 4.7 - 1.9 <0.001 Placebo 425 - 2.8 — — EVOLVE - 2 6 months 120 mg SC QM MMD (change from baseline during treatment) 231 - 4.3 - 2 <0.001 Placebo 461 - 2.3 — — Nurtec ODT rimegepant Study 1 12 wks 75 mg ODT QOD MMD (change from baseline during treatment) 348 - 4.3 - 0.8 0.01 Placebo 347 - 3.5 — — QULIPTA atogepant ADVANCE 12 wks 10 mg ODT OD MMD (change from baseline across 12wk treatment) 214 - 3.7 - 1.2 <0.001 30 mg ODT OD 223 - 3.9 - 1.4 <0.001 60 mg ODT OD 222 - 4.2 - 1.7 <0.001 Placebo 214 - 2.5 — — Vyepti eptinenzumab 12 wks 100 mg IV Q3M MMD (change from baseline across 12wk treatment period) 221 - 3.9 - 0.7 0.018 300 mg IV Q3M 222 - 4.3 - 1.1 <0.001 Placebo 222 - 3.2 Other Phase 3 Trials for CGRPs in Episodic Migraine Not intended for cross - trial comparisons Sources: Individual product labels and FDA summary basis of approvals; Neurol Ther . (2021) 10:469 – 497

17 ABP - 450 Has a Favorable Safety Profile AE Summary Placebo (N=97) Number of patients (% of patients) ABP - 450 150 Units (N=99) Number of patients (% of patients) ABP - 450 195 Units (N=109) Number of patients (% of patients) Patients with Treatment - emergent Adverse Event ( TEAE ) 57 (58.8) 54 (54.5) 59 (54.1) Patients With Serious TEAE (SAE) 2 (2.1) 3 (3.0) 1 (0.9) Patients With Treatment - related SAEs 0 1 (1.0) 0 Patients with Treatment - related TEAEs 7 (7.2) 13 (13.1) 11 (10.1) Migraine 0 0 3 (2.8) Muscular weakness 0 1 (1.0) 2 (1.8) Eyelid ptosis 1 (1.0) 1 (1.0) 1 (0.9) Injection site 0 0 2 (1.8) Neck pain 1 (1.0) 1 (1.0) 1 (0.9)

18 Efficacy Results from Phase 2 with ABP - 450 in Episodic Migraine Primary Endpoint - mean change from baseline in monthly migraine days (MMD) at weeks 21 - 24 Key Secondary and Exploratory Endpoint – Statistically significant • Treatment effect (vs. placebo): – 4.2 days placebo – 4.8 days for 150 U dose ( - 0.6 days placebo - adjusted; p=0.2844) – 5.0 days for 195 U dose ( - 0.8 days placebo - adjusted; p=0.1711) • Over time, both doses numerically separate from placebo starting at week 4 • Evidence of dose response favoring the 195 U arm • Durability over the 3 - month period (weeks 13 - 24) supports utilization as primary endpoint in Phase 3 • ≥ 75% responder rate : – 23% placebo – 37% for 150 U dose ( p=0. 0245 ) – 34% for 195 U dose ( p=0. 0439 ) • Patient Global Impression of Severity (PGI - S): – - 0.6 placebo – - 0.9 for 150 U dose ( p=0. 0436 ) – - 1.0 for 195 U dose ( p=0. 0028 ) • ≥ 50% responder rate: – 23% placebo – 59% for 150 U dose ( p=0. 2459) – 69% for 195 U dose ( p=0. 0132)

19 Actual Results vs. Simulated Sample Size Endpoints Actual Phase 2 Data Simulated Sample Size* 150U vs. Pbo (n: 92 vs. 90) 195U vs. Pbo (n: 96 vs. 90) 195U vs. Pbo (n: 200 vs. 200) 195U vs. Pbo (n: 400 vs. 400) Primary MMD at weeks 21 - 24 - 0.6 (p=0.2844) - 0.8 (p=0.1711) p=0.0409 p=0.0039 Post - hoc MMD at weeks 13 - 24 - 0.6 (p=0.1871) - 0.7 (p=0.1094) p=0.0356 p=0.0030 Secondary MHD at weeks 21 - 24 - 0.4 (p=0.5118) - 1.0 (p=0.1182) p=0.0200 p=0.0010 Post - hoc MHD at weeks 13 - 24 - 0.7 (p=0.1907) - 0.9 (p=0.0564) p=0.0160 p=0.0007 *Simulated p - values could meet statistical significance < 0.05 • Increasing the sample size to 200 and 400 patients per arm would increase the statistical power

20 Next Steps and Upcoming Events Phase 2 in Chronic Migraine Considerations for Phase 3 in Episodic Migraine Enrollment now ~430 patients and expect to complete enrollment of 465 patients in Q4 Top - line results expected in 2H 2024 Differences from Phase 2 in episodic migraine: – Higher number of patients per arm improves statistical power (~155 vs. ~90) – Higher number of monthly migraine days at baseline (~17 vs. ~9 ) – more room to improve – Likely to include more treatment - experienced patients to lower the placebo - effect Plan to request End - of - Phase 2 meeting with FDA and conduct in 1H 2024 Anticipate initiating P3 program in 2H 2024 after results from P2 in chronic migraine Likely to include only higher dose 195U (1:1 randomization) ~400 patients per arm To reduce placebo effect, the Company will require patients to have failed at least 1 prior preventive regimen To reduce placebo effect, the Company will require patients with at least 3 years of migraine history Primary endpoint likely to be reduction in MMD over the 2 nd treatment period (weeks 13 - 24)

Thank You
Exhibit 99.3

Corporate Presentation October 2023

2 Forward Looking Statements This presentation includes forward - looking statements . All statements other than statements of historical facts contained in this presentation, including statements concerning possible or assumed future actions, business strategies, events or results of operations, and any statements that refer to projections, forecasts or other characterizations of future events or circumstances, including any underlying assumptions, are forward - looking statements . These statements may involve known and unknown risks, uncertainties and other important factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward - looking statements . These statements may be preceded by, followed by or include the words “believes”, “estimates”, “expects”, “projects”, “forecasts”, “may”, “will”, “should”, “seeks”, “plans”, “scheduled”, “anticipates” or “intends” or similar expressions . The forward - looking statements in this presentation are only predictions . We have based these forward - looking statements largely on our current expectations and projections about future events and financial trends that we believe may affect our business, financial condition and results of operations . These forward - looking statements are based upon estimates and assumptions that, while considered reasonable by AEON and its management, are inherently uncertain . Factors that may cause actual results to differ materially from current expectations include, but are not limited to : (i) the outcome of any legal proceedings that may be instituted against AEON or others following the announcement of the business combination and any definitive agreements with respect thereto ; (ii) the ability to meet continued stock exchange listing standards following the consummation of the business combination ; (iii) the risk that the business combination disrupts current plans and operations of AEON as a result of the announcement and consummation of the business combination ; (iv) the ability to recognize the anticipated benefits of the business combination, which may be affected by, among other things, competition, the ability of AEON to grow and manage growth profitably, maintain relationships with customers and suppliers and retain its management and key employees ; (v) costs related to the business combination and being a public company ; (vi) changes in applicable laws or regulations ; ( vii) the possibility that AEON may be adversely affected by other economic, business, regulatory, and/or competitive factors ; (viii) AEON’s estimates of expenses and profitability ; (ix) the evolution of the markets in which AEON competes ; (x) the ability of AEON to implement its strategic initiatives, including the continued development of ABP - 450 ; (xi) the ability of AEON to defend its intellectual property ; (xii) the ability of AEON to satisfy regulatory requirements ; (xiii) the impact of adverse geopolitical and macroeconomic developments, such as the COVID - 19 pandemic, the Israel - Hamas conflict, the Ukraine - Russia conflict and related sanctions, actual and anticipated changes in interest rates, economic inflation and the responses by central banking authorities to control such inflation on AEON’s business ; (xiv) AEON’s expected capital resources and liquidity needs ; and (xv) other risks and uncertainties set forth in the section entitled "Risk Factors" and "Cautionary Note Regarding Forward - Looking Statements" in the company’s final proxy statement/prospectus relating to the business combination . Because forward - looking statements are inherently subject to risks and uncertainties, some of which cannot be predicted or quantified and some of which are beyond our control, you should not rely on these forward - looking statements as predictions of future events . The events and circumstances reflected in our forward - looking statements may not be achieved or occur, and actual results could differ materially from those projected in the forward - looking statements . Moreover, we operate in an evolving environment and a competitive industry . New risks and uncertainties may emerge from time to time, and it is not possible for management to predict all risks and uncertainties, nor can we assess the impact of all factors on our business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward - looking statements we may make in this presentation . As a result of these factors, although we believe that the expectations reflected in our forward - looking statements are reasonable, we cannot assure you that the forward - looking statements in this presentation will prove to be accurate . Except as required by applicable law, we do not plan to publicly update or revise any forward - looking statements contained herein, whether as a result of any new information, future events, changed circumstances, or otherwise . We qualify all of our forward - looking statements by these cautionary statements . You should view this presentation completely and with the understanding that the actual future results, levels of activity, performance, events and circumstances of AEON may be materially different from what is expected .

3 Investment Highlights Botulinum toxin has demonstrated utility across dozens of published uses expected to be accessible to ABP - 450; accelerated and simplified commercialization timeline due to existing aesthetic BLA (separately held by Evolus) and manufacturing site approved by FDA, EMA and Health Canada Episodic migraine approval would nearly triple the current addressable patient population (Botox ® indicated for chronic migraine only); ABP - 450 Phase 2 migraine study includes chronic and episodic migraine patients with a streamlined injection protocol with potential to enhance safety and tolerability Potential to pursue traditional pharma pricing model currently not pursued by therapeutic toxin competition with a 900 kDa botulinum toxin expected to facilitate physician adoption Significant neurotoxin commercial and clinical development experience among management team translating to approximately $162M invested in AEON since 2019 Strong Potential Episodic Migraine Market Expansion Business Model Advantage Strong Leadership & Sponsorship Market Ripe for Competition Single existing competitor for key target markets (episodic & chronic migraine); unlike in aesthetic market, ABP - 450’s therapeutic focus will compete with market leader on a product - to - product basis, not against a portfolio of products PTSD Opportunity Ongoing pre - clinical program utilizing proprietary injection paradigm in a novel part of the anatomy is designed to provide IND supporting safety and efficacy data; this innovative approach has the potential for utility across a broad Neuro/Psych portfolio including PTSD

4 Leadership Team with Highly Relevant Industry Experience and Track Record of Success Experienced Management Team Marc Forth Chad Oh, MD Chief Executive Officer Chief Medical Officer • 25+ years of Biopharma experience • Former US Business Lead for BOTOX ® Therapeutic • 16 years at Allergan dedicated to the entire BOTOX ® franchise • 7 years at TAP Pharmaceuticals responsible for Lupron Depot (Urology, Oncology and Gynecology) • 30+ years of combined experience in academia and the pharmaceutical industry • Responsible for multiple IND, NDA, and BLA submissions • Chief, Division of Allergy and Immunology at Harbor - UCLA Medical Center • Associate Professor, Department of Pediatrics at UCLA School of Medicine • Published multiple scientific papers, books, book chapters, and abstracts, including 38 peer - reviewed original scientific papers • 10+ years of legal experience in corporate governance, mergers & acquisitions and capital markets • Associate General Counsel of Glaukos Corporation, responsible for business development activities, capital markets, corporate governance and SEC reporting • Counsel at O’Melveny & Myers • B.S. in Business Management, Brigham Young University and J.D. from the UCLA School of Law EVP, Chief Legal Officer & Secretary Alex Wilson Peter Reynolds Acting Chief Financial Officer • 25+ years of financial experience in Healthcare, Medical Device, and Aesthetic Toxins • Senior Finance roles with both Publicly Traded and Privately held companies • Significant experience in mergers, acquisitions and public offerings

5 Botulinum Toxin: The Ultimate Platform Product

6 Global Therapeutic Toxin Landscape AbbVie Inc. Merz Pharma Ipsen Group Molecular Size 900 kDa 900 kDa 150 kDa ~400 kDa 150 kDa Approved Indications 1. Blepharospasm 2. Strabismus 3. Cervical Dystonia 4. Hyperhidrosis 5. Spasticity 6. Chronic Migraine 7. Overactive Bladder 8. Neurogenic Detrusor Overactivity (adult and pediatric) None 1. Blepharospasm 2. Cervical Dystonia 3. Adult Spasticity (Upper Limb) 4. Chronic Sialorrhea 1. Cervical Dystonia 2. Spasticity 1. Cervical Dystonia In Development 1. Atrial Fibrillation 2. Episodic Migraine 3. Essential Tremor 4. IC/BPS 1. Migraine (episodic & chronic) 2. Cervical Dystonia 3. Gastroparesis 4. Posttraumatic Stress Disorder (PTSD) Undisclosed 1. Neurogenic Detrusor Overactivity 1. Adult Spasticity (Upper Limb) FDA Approved US Share 95% 2% 2% Sources: Decision Resources Group Therapeutic Botulinum Toxin Market Analysis Global 2021

7 Indication Current Phase 2020 2021 2022 2023 2024 Recent/Upcoming Milestones 1H 2H 1H 2H 1H 2H 1H 2H 1H 2H ABP - 450 Episodic Migraine 1 Phase 2 ongoing x IND accepted Oct 2020 x First patient treated Mar 2021 x Enrollment completed Dec 2022 • P2 data - Fall 2023 Chronic Migraine 2 x IND accepted Oct 2020 x First patient treated Mar 2021 • P2 data anticipated 2H 2024 Cervical Dystonia Phase 2 completed x IND accepted Sep 2020 x First patient treated Apr 2021; last patient last visit Jul 2022 x P2 data reported Sep 2022 • P3 initiation anticipated 2024 Gastroparesis Phase 2 ready x IND accepted 2022 Posttraumatic Stress Disorder Preclinical x Safety assessment ongoing ABP - 450 Indications: Pipeline in a Product 1. Episodic: <15 headache days AND 6 - 14 migraine days / month 2. Chronic: >15 headache days AND >8 migraine days / month

8 Global Therapeutic Toxin Market – 9.9% Projected Growth Through 2027 • Current indications: Organic growth in current indications driven primarily by continued investment in disease awareness and growing patient populations • New indications: Development in therapeutic specialties that do not currently have a toxin treatment option • Improved reimbursement: Favorable dynamics to facilitate coverage at current and projected pricing levels Anticipated Volume Growth Drivers $2.3B $2.7B $3.0B $3.2B $3.5B $3.8B $4.1B $4.4B 2020A 2021E 2022E 2023E 2024E 2025E 2026E 2027E 2.7M procedures $557 ASP (US) 5.0M procedures $619 ASP (US) CGAR: 1.5% CGAR: 8.8% 9% 7% 84% EU Asia Pacific US 6% 13% 17% 28% 36% Overactive Bladder Other Cervical Dystonia Spasticity Migraine Global Therapeutic Toxin Market Share Breakdown By Geography By Indication Global Therapeutic Toxin Market Projections Source: Decision Resources Group Therapeutic Botulinum Toxin Market Analysis Global 2021

9 No competitive product has therapeutic indications under separate BLA Model Allows Reimbursement Based Solely on Therapeutic Pricing *Average selling price Value to Physician Consistent, predictable reimbursement Value to Payor Potential to offer financial incentives • Original BLA expected to allow AEON’s ASP* to be unencumbered by pricing pressures from aesthetic indications that hamper the competition’s reimbursement structure • Physicians to receive consistent and favorable reimbursement from payors • Flexibility to provide targeted economic incentives to payors and/or providers that competition cannot

(episodic and chronic prophylaxis) Migraine

11 Migraine Market Resurgence From New Players is Benefitting Toxins New CGRPs are rapidly expanding the market driven by new product launches and promotional investment Migraine affects ~40M people in the United States & ~1B people worldwide every year, making it the third most prevalent illness in the world 1 Chronic Migraine • 15+ headache days/month • ~4.0M patients ($11.2B market) 2 Episodic Migraine • 6 - 14 headache days/month • ~9.4M patients ($18.5B market) 3 Accelerating Migraine Market • Botox ® in chronic migraine returned to double digit growth after a brief flat period due to CGRP launches and COVID challenges • Botox ® only has a claim for chronic migraine vs. CGRPs with both chronic and episodic indications Toxins are Faring Well Despite Competition • Pursuing label for broader patient population than Botox ® with inclusion of both episodic and chronic migraine patients in Phase 2 • Novel injection paradigm with fewer injections and differentiated injection locations for ABP - 450 • Potential for increased safety and tolerability • High overlap in commercial audience between migraine and cervical dystonia ABP - 450 Opportunity 1. Migraine Research Foundation. 2. Company estimates based on 2017 US Census Projections; Diamond, Patterns of Diagnosis and Acute and Preventive Treatment for Mig raine in the United States: Results from the American Migraine Prevalence and Prevention Study (2006); Lipton, Barriers to the Diagnosis and Treatment of Migraine (2012) and assumes 2.2 million diagn ose d patients receiving four treatments per year (two vials) at a cost of $634 per vial 3. Messali, Direct and Indirect Costs of Chronic and Episodic Migraine in the United States: A Web - Based Survey (2016) and assumes 3.65 million diagnosed patients receiving four treatments per year (two vials) at a cost of $634 per vial. 4. DRG report, Migraine Disease Landscape & Forecast, December 2020

12 Q1 2019 Q2 2019 Q3 2019 Q4 2019 Q1 2020 Q2 2020 Q3 2020 Q4 2020 Q1 2021 Q2 2021 Q3 2021 Q4 2021 Q1 2022 Q2 2022 Q3 2022 Q4 2022 Normalized Botox 560,178 591,747 596,955 603,957 571,818 562,773 617,901 638,988 656,238 709,350 728,967 733,767 755,091 777,729 797,475 769,050 CGRPs 252,687 365,078 466,273 530,906 565,375 656,832 678,583 704,068 725,935 773,386 784,708 792,707 804,160 856,029 897,106 924,526 K 100K 200K 300K 400K 500K 600K 700K 800K 900K 1000K Volume (# of Claims) NORMALIZED Botox and CGRPs in Preventive Migraine Treatment [Q1’19 - Q4’22] Botox Still Showing Impressive YoY Growth Despite New CGRPs Source: KOMODO Claims Data (2015 - Dec'2022) CGRP includes Aimovig, Ajovy, Emgality,Vyepti, Qulipta Normalized Botox claims = Botox claims * 3 Competitive products listed at time of FDA approval +9% +10% +15% +15% +18% +26% +15% +6% +4% - 5% +2% Qulipta Vyepti +5% Nurtec ODT Prophylaxis

13 Addressable Patient Population ~3x Higher with Episodic Indication 1.6M Total Addressable Patients 260M People Estimated US 18+ Population 40M Patients (15%) Estimated Migraine and severe HA Patients 9.4M Patients (24%) Episodic Migraine (6 - 14 HA/month) 4.0M Patients (10%) Chronic Migraine (15+ HA/month) 2.2M Patients (56%) Diagnosed Prevalence 3.7M Patients (39%) Diagnosed Prevalence 820k Patients (37%) Treated Patients (Prophylactic) 740k Patients (20%) Treated Patients (Prophylactic) Chronic Migraine Episodic Migraine Sources: 2017 US Census Projections Burch, The Prevalence and Impact of Migraine and Severe Headache in the United States: Figures and Trends From Government Hea lth Studies (2018) Lipton, Migraine in America Symptoms and Treatment (MAST) Study: Baseline Study Methods, Treatment Patterns, and Gender Diffe ren ces (2018) Buse, Impact of Migraine on the Family: Perspectives of People With Migraine and Their Spouse/Domestic Partner in the CaMEO S tud y (2016) Diamond, Patterns of Diagnosis and Acute and Preventive Treatment for Migraine in the United States: Results from the America n M igraine Prevalence and Prevention Study (2006) Messali, Direct and Indirect Costs of Chronic and Episodic Migraine in the United States: A Web - Based Survey (2016)

14 • N = 765 • ~60 sites in US, Canada & Australia • Includes both EM & CM patients • # headache days and migraine days/month established during 4 - week baseline prior to randomization • 3 arms: 150 Units, 195 Units, PBO • 2 injection cycles, 3 months apart • 6 - month treatment duration • Novel injection paradigm: - 22 injection sites (ABP - 450 low dose) - vs. 31 injections for Botox Primary: • Mean change of monthly migraine days (MMD) at Week 24 • Incidence of TEAEs throughout study compared to placebo Secondary: • Percentage of patients with reduction from baseline of ≥50%, 75%, 100% in average number of MMD throughout the study • Change in use of rescue medications from baseline • Safety endpoints of change in laboratory tests, ECG, etc. Exploratory: • Change in PGI - S, PGI - C, MIDAS, etc. Placebo n= 255 195 Units ABP - 450 n= 255 24 weeks Primary Efficacy Endpoint 150 Units ABP - 450 n= 255 4 - week Baseline 4 - week Screening Randomized R Endpoints Randomized Double - Blinded Placebo - Controlled Study Open Label Extension Study 4 treatments of ABP - 450 52 weeks Study Design 12 weeks Phase 2 Design: Episodic Migraine (EM) and Chronic Migraine (CM)

15 Independent Analysis of Phase 2 Episodic and Chronic Cohorts Randomization and Stratified for Episodic Migraine and Chronic Migraine Episodic Migraine N=~300 <15 headache days / month And 6 - 14 migraine days / month 150 U N= 99 195 U N=108 Placebo N= 98 Chronic Migraine N=~465 ≥ 15 headache days / month And >8 migraine days / month 150 U N=155 195 U N=155 Placebo N=155 Final Analysis of the Episodic Cohort Fall 2023 Final Analysis of the Chronic Cohort Anticipated 2H 2024

16 26 injection sites* (195 Units) in P2 migraine protocol focused on specific nerves vs. 39 with Botox (195 units) targeting muscles Smart Injection Paradigm Targeting Nerves - Differentiation from Botox *22 injection sites in low dose (150 Units)

17 Phase 3 Trials for CGRPs in Episodic Migraine Not intended for cross - trial comparisons; Sources: package inserts; Neurol Ther (2021) 10:469 – 497 Brand Generic Company Trial Duration Dose Primary Endpoint N Change (days) Difference from placebo p - value Aimovig erenumab STRIVE 24 Weeks 70 mg SC QM Monthly migraine days (change from baseline to months 4 through 6) 312 - 3.2 - 1.4 <0.001 140 mg SC QM 318 - 3.7 - 1.9 <0.001 Placebo 316 - 1.8 — — ARISE 12 weeks 70 mg SC QM Monthly migraine days (change from baseline in the last 4 weeks of the trial) 282 - 2.9 - 1.1 <0.001 Placebo 288 - 1.8 — — Ajovy fremanezumab 12 weeks 225 mg SC QM Monthly migraine days (change during the 12 - week trial period, after first dose) 287 - 3.7 - 1.5 <0.001 675 mg SC Q3M 288 - 3.4 - 1.2 <0.001 Placebo 290 - 2.2 — — Emgality galcanezumab EVOLVE - 1 6 months 120 mg SC QM Monthly migraine days (change from baseline during the treatment period) 210 - 4.7 - 1.9 <0.001 Placebo 425 - 2.8 — — EVOLVE - 2 6 months 120 mg SC QM Monthly migraine days (change from baseline during the treatment period) 231 - 4.3 - 2.0 <0.001 Placebo 461 - 2.3 — — Nurtec ODT rimegepant Study 1 12 weeks 75 mg ODT QOD Monthly migraine days (change from baseline during the treatment period) 348 - 4.3 - 0.8 0.010 Placebo 347 - 3.5 — — QULIPTA atogepant ADVANCE 12 weeks 10 mg ODT OD Monthly migraine days (change from baseline across 12 - week treatment period) 214 - 3.7 - 1.2 <0.001 30 mg ODT OD 223 - 3.9 - 1.4 <0.001 60 mg ODT OD 222 - 4.2 - 1.7 <0.001 Placebo 214 - 2.5 — —
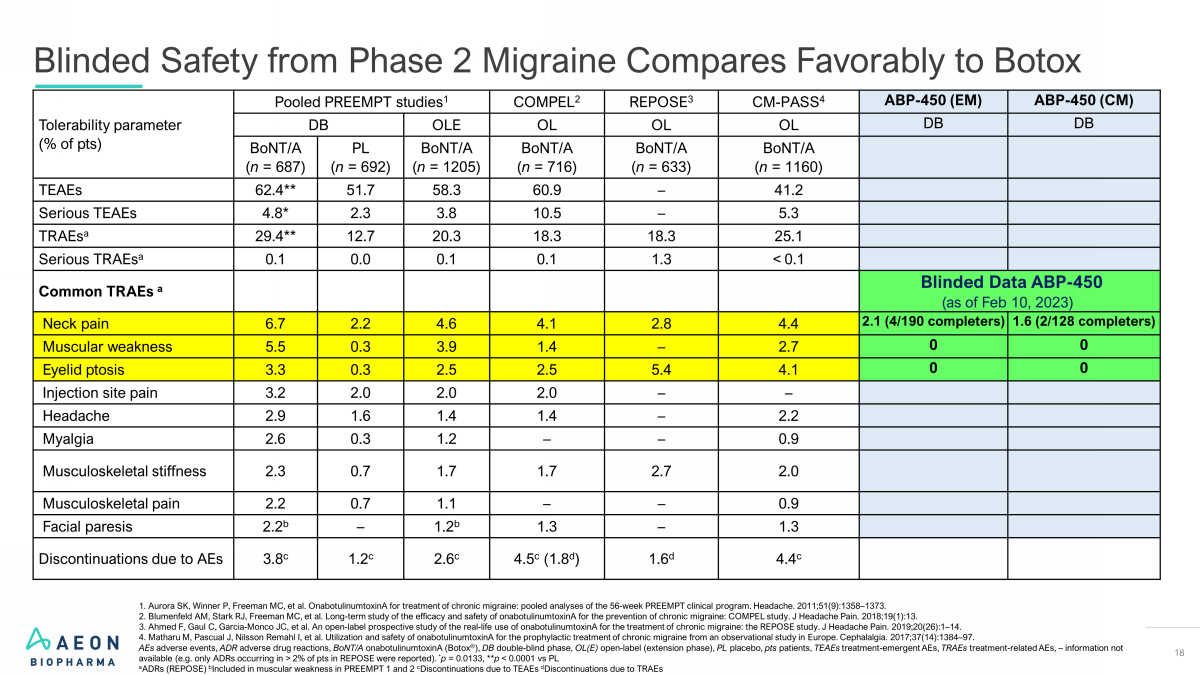
18 Tolerability parameter (% of pts) Pooled PREEMPT studies 1 COMPEL 2 REPOSE 3 CM - PASS 4 ABP - 450 (EM) ABP - 450 (CM) DB OLE OL OL OL DB DB BoNT/A ( n = 687) PL ( n = 692) BoNT/A ( n = 1205) BoNT/A ( n = 716) BoNT/A ( n = 633) BoNT/A ( n = 1160) TEAEs 62.4** 51.7 58.3 60.9 – 41.2 Serious TEAEs 4.8* 2.3 3.8 10.5 – 5.3 TRAEs a 29.4** 12.7 20.3 18.3 18.3 25.1 Serious TRAEs a 0.1 0.0 0.1 0.1 1.3 < ௗ 0.1 Common TRAEs a Blinded Data ABP - 450 (as of Feb 10, 2023) Neck pain 6.7 2.2 4.6 4.1 2.8 4.4 2.1 (4/190 completers) 1.6 (2/128 completers) Muscular weakness 5.5 0.3 3.9 1.4 – 2.7 0 0 Eyelid ptosis 3.3 0.3 2.5 2.5 5.4 4.1 0 0 Injection site pain 3.2 2.0 2.0 2.0 – – Headache 2.9 1.6 1.4 1.4 – 2.2 Myalgia 2.6 0.3 1.2 – – 0.9 Musculoskeletal stiffness 2.3 0.7 1.7 1.7 2.7 2.0 Musculoskeletal pain 2.2 0.7 1.1 – – 0.9 Facial paresis 2.2 b – 1.2 b 1.3 – 1.3 Discontinuations due to AEs 3.8 c 1.2 c 2.6 c 4.5 c (1.8 d ) 1.6 d 4.4 c 1. Aurora SK, Winner P, Freeman MC, et al. OnabotulinumtoxinA for treatment of chronic migraine: pooled analyses of the 56 - week PREEMPT clinical program. Headache. 2011;51(9):1358 – 1373. 2. Blumenfeld AM, Stark RJ, Freeman MC, et al. Long - term study of the efficacy and safety of onabotulinumtoxinA for the preventi on of chronic migraine: COMPEL study. J Headache Pain. 2018;19(1):13. 3. Ahmed F, Gaul C, Garcia - Monco JC, et al. An open - label prospective study of the real - life use of onabotulinumtoxinA for the t reatment of chronic migraine: the REPOSE study. J Headache Pain. 2019;20(26):1 – 14. 4. Matharu M, Pascual J, Nilsson Remahl I, et al. Utilization and safety of onabotulinumtoxinA for the prophylactic treatment of chronic migraine from an observational study in Europe. Cephalalgia. 2017;37(14):1384 – 97. AEs adverse events, ADR adverse drug reactions, BoNT/A onabotulinumtoxinA (Botox ® ), DB double - blind phase, OL(E) open - label (extension phase), PL placebo, pts patients, TEAEs treatment - emergent AEs, TRAEs treatment - related AEs, – information not available (e.g. only ADRs occurring in > ௗ 2% of pts in REPOSE were reported). * p = 0.0133, ** p < 0.0001 vs PL a ADRs (REPOSE) b Included in muscular weakness in PREEMPT 1 and 2 c Discontinuations due to TEAEs d Discontinuations due to TRAEs Blinded Safety from Phase 2 Migraine Compares Favorably to Botox

Gastroparesis

20 Gastroparesis Opportunity for ABP - 450 • 2019 FDA Guidance for Industry 1 • Since a well - defined and reliable patient reported outcome (PRO) is not yet available, FDA recommends that the core signs and symptoms be included as endpoints. • Anticipate initiating a Phase 2a study in 2024 • Our primary endpoint measures change in core signs and symptoms from baseline over a 12 - week treatment period • We plan to assess idiopathic and diabetic patients in separate trials Potential Regulatory Pathway • Defined by delayed gastric emptying • Symptoms are chronic with episodic exacerbations • Nausea, vomiting and pain are most troubling symptoms • Both idiopathic and diabetic (nerve damage leads to impaired intestinal muscle function) • Very limited therapeutic options; Reglan ® and Gimoti tm (metoclopramide) limited by AEs The Disorder • ~400,000 patients 2 • ~$900M market • High unmet need, low competitive intensity • We are aware of no other neurotoxin pursuing gastroparesis indication • Data from investigator - sponsored trials show positive response to neurotoxins with endoscopic intrasphincter injection of the pylorus in patients with idiopathic and diabetic gastroparesis ABP - 450 Opportunity 1. https://www.fda.gov/media/129880/download 2. Company estimates based on 2017 US Census Projections; Syed, Epidemiology and Diagnosis of Gastroparesis in the United States : A Population - based Study. (2019); and Parkman, Clinical features of idiopathic gastroparesis vary with sex, body mass, symptom onset, delay in gastric emptying, and gastroparesis severity (2011).

21 Provides an Opportunity for a Targeted Treatment for Gastroparesis Injections in the Pylorus and Pyloric Sphincter Region Sclerotherapy needle Esophagogastroduodenoscopy Plan to administer injections of ABP - 450 using a standard sclerotherapy needle in the pylorus and pyloric sphincter region Esophagus Lower Esophageal Sphincter Pyloric Sphincter Duodenum • Initiated preclinical study Dec 2020; completed Sep 2021 • IND accepted May 2022

Posttraumatic Stress Disorder (PTSD)

23 Posttraumatic Stress Disorder (PTSD) • PTSD is well defined with broad disease awareness • A psychiatric disorder that may occur in people who experience or witness a traumatic event or events • Categories of symptoms include intrusion (involuntary memories), avoidance, alterations in cognition and mood (negative thoughts and feelings), and alterations in arousal and reactivity (angry outbursts) The Disorder 1 • Current t reatments include cognitive behavioral therapy, medication (e.g., SSRIs, SNRIs), and other alternative therapies • Established FDA regulatory pathway for clinical development with several medications approved for use, including Zoloft and Paxil • Numerous validated scales are already widely accepted (e.g., CAPS, PCL - 5, BDI) Current Treatments & Regulatory Pathway 1. American Psychiatric Association. https://www.psychiatry.org/patients - families/ptsd/what - is - ptsd .

24 Posttraumatic Stress Disorder Associated with the Stellate Ganglion Source: Image Left: Rae Olmsted KL, Bartoszek M, Mulvaney S, et al. Effect of Stellate Ganglion Block Treatment on Posttraumatic Stre ss Disorder Symptoms: A Randomized Clinical Trial. JAMA Psychiatry. 2020;77(2):130 – 138. doi:10.1001/jamapsychiatry.2019.3474. Image Right: Levi, Ofir, Ariel Ben Yehuda, Daniel S. Pine, and Yair Bar - Haim. “A Sobering Look at Treatment Effectiveness of Mil itary - Related Posttraumatic Stress Disorder.” Clinical Psychological Science 10, no. 4 (2021): 690 – 99. https://doi.org/10.1177/21677026211051314. Effect of Stellate Ganglion Block Treatment on Posttraumatic Stress Disorder Symptoms A Randomized Clinical Trial Kristine L. Rae Olmsted, MSPH; Michael Bartoszek, MD; Sean Mulvaney, MD; et al JAMA Psychiatry. 2020;77(2):130 - 138. Key Points Question : How does stellate ganglion block compare with sham treatment in reducing the severity of posttraumatic stress disorder symptoms over 8 weeks? Findings : In this sham - controlled randomized clinical trial, 2 stellate ganglion block treatments 2 weeks apart were effective in reducing Clinician - Administered PTSD Scale for DSM - 5 total symptom severity scores over 8 weeks . The adjusted mean symptom change was − 12 . 6 points for the group receiving stellate ganglion blocks, compared with − 6 . 1 points for those receiving sham treatment, a significant difference . Meaning : Stellate ganglion block treatment warrants further study as a posttraumatic stress disorder treatment adjunct . A Sobering Look at Treatment Effectiveness of Military - Related Posttraumatic Stress Disorder A Randomized Clinical Trial Ofir Levi, Ariel Ben Yehuda, Yair Bar - Haim; et al Clinical Psychological Science. 2021; 10 , no.4 Abstract Approximately two thirds of veterans with posttraumatic stress disorder (PTSD) remain with the disorder following treatment . Pinpointing the per - symptom effectiveness of treatments in real - world clinical settings can highlight relevant domains for treatment augmentation and development . Baseline and posttreatment assessments of PTSD and depression were performed in 709 veterans with PTSD . PTSD remission was 39 . 4 % . Treatment was least effective for intrusion symptoms and had no effect on flashbacks or on poor recall of traumatic features . Of veterans who remitted, 72 . 8 % still met diagnostic criteria for at least one cluster . Poor clinical effectiveness was noted for depression ; only 4 . 1 % of the patients remitted following treatment . Treatments for veterans with PTSD show limited overall effectiveness in real - world settings . Enhancing treatment response may require enhancing provider fidelity and patient compliance with extant treatments or the development of new treatments that specifically target the symptoms of PTSD that do not respond well to extant treatments .

25 Stellate ganglion (sympathetic) block using ultrasound guidance • Establish safety and preliminary efficacy signal • Rats placed in supine position under anesthesia • Administer approximately 10 - 20 µl of active, following standard protocols • Observe for 1 - 2 weeks after the injection • Monitor heart rate and blood pressure • Assess effect on sympathetic nervous pathway ABP - 450 Pre - Clinical PTSD Study

Cervical Dystonia
27 Cervical Dystonia Opportunity for ABP - 450 • Potential for efficient development • Potential to allow participation in segment of on - label movement disorders • Potential to leverage into a broader muscle spasticity indication and label with a focused clinical program Important Indication for Muscle Movement Disorders • Cervical dystonia is a chronic condition with no cure • Painful and debilitating twisting movements of neck and shoulders • Botulinum toxin injection is the standard of care • Established outcome measures and regulatory pathway The Disorder • ~50,000 patients • ~$360M market • Approximately 40% of therapeutic toxin market sales in 2019 were for various muscle movement disorders • Anticipate that Phase 3 program will include a head - to - head comparison to Botox ® to demonstrate non - inferiority US Market Opportunity For ABP - 450 Sources: Company estimates based on 2017 US Census Projections Defazio, Descriptive Epidemiology of Cervical Dystonia (2013) Richardson, American Academy of Neurology - Dystonia Treatment (2017)

28 Open Label Extension Proposed to Occur in Parallel with Phase 3 Trial Cervical Dystonia Phase 2 Study Design - Dose Ranging • First patient dosed April 2021 • Phase 2 top line data reported in September 2022 Randomized Double - Blinded Placebo - Controlled Study 20 weeks Randomized R 1 - week baseline 16 - week washout of prior toxin treatment Open Label Extension Study Placebo n= 15 150 Units ABP - 450 n= 15 250 Units ABP - 450 n= 15 350 Units ABP - 450 n= 15 4 treatments of ABP - 450 52 weeks Primary: • Safety of ABP - 450 Secondary: • Change in TWSTRS • PGI - C and CGI - C • PGI - S and CGI - S Exploratory: • C - SSRS • Dysphagia Score Endpoints • N = 60 • 40 sites in US • 3 doses; 4 arms • 1 injection in randomized portion • 4 injections in OLE • 20 - week primary endpoint • 72 weeks total Study Design

29 Phase 2 Data Conclusions • Phase 2 trial met primary and other key endpoints, supporting the safety and efficacy of ABP - 450 in reducing signs and symptoms associated with CD. • ABP - 450 demonstrated adverse event rates similar to, or lower than, other botulinum toxin products for the treatment of CD. • Zero discontinuations due to Treatment - Emergent Adverse Events (TEAEs) • Low rate of treatment - related TEAEs (TRAEs) • Zero dysphagia cases in the 150 U arm and low rate of dysphagia (11%) and muscle weakness (6.7%) overall • All TRAEs were mild to moderate in severity and transient in nature • ABP - 450 demonstrated efficacy similar to, or better than, other botulinum toxin products for the treatment of CD. • TWSTRS at Week 4 improved 14.01 points in 150 U; 11.28 points in 250 U; 9.92 points in 350 U; 3.57 points in placebo – Statistical significance in lower dose arms (150 U and 250 U) vs. placebo and numerical improvement in high dose arm (350 U) vs. placebo • Patient Global Impression of Change (PGI - C) demonstrated statistically significant improvement in all three ABP - 450 dose groups over placebo • Clinical Global Impression of Change (CGI - C) demonstrated statistically significant improvement in all three ABP - 450 dose groups over placebo • Median duration of treatment effect was at least 20 weeks for 150 U, 20 weeks for 250 U, and 20 weeks for 350U.

Financial Overview

31 Financial Overview Sufficient capital to fund operations beyond topline data from ongoing Phase 2 study of ABP - 450 for episodic migraine in Fall 2023 $0 D ebt 27.4M Basic Shares Outstanding $25M Cash at Close 1 14.48M Warrants 2 19.45M Total Potential Earnout Shares 1. Proforma as of 7 - 24 - 23 2. 9.2M warrants with $11.50 strike and 5.28M warrants with $8.05 strike 3. Approximately 7.5M shares subject to forward purchase agreement; for purchase details, see SEC filings ~7.5M Shares in Forward Purchase Agreement for potential purchase 3

32 ABP - 450 – Clinical and Regulatory Timeline 2025 2H 1H 2026 2H 1H 2027 2H 1H 2028 2H 1H 2029 2H 1H Earnout Deadline Chronic Migraines Episodic Migraines Cervical Dystonia 14.45M 5 M 2M shares - upon first patient dosed in Phase 3 study in the first to occur between CM or EM prior to 06/30/25 2024 2H 1H Aligns AEON and SPAC Sponsor Incentives with Public Market Investors Earnout Structure Note: CM = Chronic Migraine, EM = Episodic Migraine, CD = Cervical Dystonia. Please refer to “ Forward - Looking Statements” in th e slide titled "Disclaimer" for important information you should consider regarding the timing of earn - out milestone achievement, as no assurance can be given that any such indicated earn - out milestone will be achieved on the timeline indicated or at all. 1. If BLA acceptance for episodic migraine occurs prior to BLA acceptance for chronic migraine, earnout for episodic migraine BL A a cceptance will increase from 4M shares to 11M shares and there shall be no further earnout issuance for chronic migraine. In the event that AEON licenses any of its products (except for Migraine or CD indications) to a third - party licensor for distribution in the U.S. market prior to the time that the 11M shares have been issued upon achievement of either the BLA acceptance for episodic migraine or chronic migraine (as described above), then 2M shares shall be issued upon the entry int o such license agreement and the remaining shares to be issued for achievement of the BLA acceptance for episodic migraine or chronic migraine, as applicable, will be correspondingly reduced. 2. 1.45M founder shares shall vest upon the earlier to occur of (i) BLA acceptance for chronic migraine or (ii) BLA acceptance f or episodic migraine, subject to potential forfeiture of sponsor shares pursuant to the Business Combination Agreement. 7M shares - upon BLA acceptance for CM prior to 06/30/28 4M shares 1 - upon BLA acceptance for EM prior to 06/30/29 1.45M shares – upon earlier of: 1) BLA acceptance for CM prior to 06/30/28 or 2) BLA acceptance for EM prior to 06/30/29 2 5M shares - upon BLA acceptance for CD prior to 11/30/26

33 Investment Highlights Botulinum toxin has demonstrated utility across dozens of published uses expected to be accessible to ABP - 450; accelerated and simplified commercialization timeline due to existing aesthetic BLA (separately held by Evolus) and manufacturing site approved by FDA, EMA and Health Canada Episodic migraine approval would nearly triple the current addressable patient population (Botox ® indicated for chronic migraine only); ABP - 450 Phase 2 migraine study includes chronic and episodic migraine patients with a streamlined injection protocol with potential to enhance safety and tolerability Potential to pursue traditional pharma pricing model currently not pursued by therapeutic toxin competition with a 900 kDa botulinum toxin expected to facilitate physician adoption Significant neurotoxin commercial and clinical development experience among management team translating to approximately $162M invested in AEON since 2019 Strong Potential Episodic Migraine Market Expansion Business Model Advantage Strong Leadership & Sponsorship Market Ripe for Competition Single existing competitor for key target markets (episodic & chronic migraine); unlike in aesthetic market, ABP - 450’s therapeutic focus will compete with market leader on a product - to - product basis, not against a portfolio of products PTSD Opportunity Ongoing pre - clinical program utilizing proprietary injection paradigm in a novel part of the anatomy is designed to provide IND supporting safety and efficacy data; this innovative approach has the potential for utility across a broad Neuro/Psych portfolio including PTSD

Thank you
v3.23.3
Cover
|
Oct. 19, 2023 |
| Document Information [Line Items] |
|
| Document Type |
8-K
|
| Amendment Flag |
false
|
| Document Period End Date |
Oct. 19, 2023
|
| Entity File Number |
001-40021
|
| Entity Registrant Name |
AEON Biopharma, Inc.
|
| Entity Central Index Key |
0001837607
|
| Entity Tax Identification Number |
85-3940478
|
| Entity Incorporation, State or Country Code |
DE
|
| Entity Address, Address Line One |
5
Park Plaza
|
| Entity Address, Address Line Two |
Suite 1750
|
| Entity Address, City or Town |
Irvine
|
| Entity Address, State or Province |
CA
|
| Entity Address, Postal Zip Code |
92614
|
| City Area Code |
949
|
| Local Phone Number |
354-6499
|
| Written Communications |
false
|
| Soliciting Material |
false
|
| Pre-commencement Tender Offer |
false
|
| Pre-commencement Issuer Tender Offer |
false
|
| Entity Emerging Growth Company |
true
|
| Elected Not To Use the Extended Transition Period |
false
|
| Common Stock [Member] |
|
| Document Information [Line Items] |
|
| Title of 12(b) Security |
Class A Common Stock, $0.0001 par value per share
|
| Trading Symbol |
AEON
|
| Security Exchange Name |
NYSE
|
| Warrant [Member] |
|
| Document Information [Line Items] |
|
| Title of 12(b) Security |
Warrants
to purchase Class A common stock
|
| Trading Symbol |
AEON
WS
|
| Security Exchange Name |
NYSE
|
| X |
- DefinitionBoolean flag that is true when the XBRL content amends previously-filed or accepted submission.
| Name: |
dei_AmendmentFlag |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionFor the EDGAR submission types of Form 8-K: the date of the report, the date of the earliest event reported; for the EDGAR submission types of Form N-1A: the filing date; for all other submission types: the end of the reporting or transition period. The format of the date is YYYY-MM-DD.
| Name: |
dei_DocumentPeriodEndDate |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:dateItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe type of document being provided (such as 10-K, 10-Q, 485BPOS, etc). The document type is limited to the same value as the supporting SEC submission type, or the word 'Other'.
| Name: |
dei_DocumentType |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:submissionTypeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 1 such as Attn, Building Name, Street Name
| Name: |
dei_EntityAddressAddressLine1 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 2 such as Street or Suite number
| Name: |
dei_EntityAddressAddressLine2 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Definition
+ References
+ Details
| Name: |
dei_EntityAddressCityOrTown |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCode for the postal or zip code
| Name: |
dei_EntityAddressPostalZipCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the state or province.
| Name: |
dei_EntityAddressStateOrProvince |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:stateOrProvinceItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionA unique 10-digit SEC-issued value to identify entities that have filed disclosures with the SEC. It is commonly abbreviated as CIK. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityCentralIndexKey |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:centralIndexKeyItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionIndicate if registrant meets the emerging growth company criteria. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityEmergingGrowthCompany |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCommission file number. The field allows up to 17 characters. The prefix may contain 1-3 digits, the sequence number may contain 1-8 digits, the optional suffix may contain 1-4 characters, and the fields are separated with a hyphen.
| Name: |
dei_EntityFileNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:fileNumberItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTwo-character EDGAR code representing the state or country of incorporation.
| Name: |
dei_EntityIncorporationStateCountryCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarStateCountryItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe exact name of the entity filing the report as specified in its charter, which is required by forms filed with the SEC. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityRegistrantName |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe Tax Identification Number (TIN), also known as an Employer Identification Number (EIN), is a unique 9-digit value assigned by the IRS. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityTaxIdentificationNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:employerIdItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionLocal phone number for entity.
| Name: |
dei_LocalPhoneNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 13e
-Subsection 4c
| Name: |
dei_PreCommencementIssuerTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14d
-Subsection 2b
| Name: |
dei_PreCommencementTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTitle of a 12(b) registered security. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b
| Name: |
dei_Security12bTitle |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:securityTitleItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the Exchange on which a security is registered. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection d1-1
| Name: |
dei_SecurityExchangeName |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarExchangeCodeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as soliciting material pursuant to Rule 14a-12 under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Section 14a
-Number 240
-Subsection 12
| Name: |
dei_SolicitingMaterial |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTrading symbol of an instrument as listed on an exchange.
| Name: |
dei_TradingSymbol |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:tradingSymbolItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as written communications pursuant to Rule 425 under the Securities Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Securities Act
-Number 230
-Section 425
| Name: |
dei_WrittenCommunications |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Details
| Name: |
us-gaap_StatementClassOfStockAxis=us-gaap_CommonStockMember |
| Namespace Prefix: |
|
| Data Type: |
na |
| Balance Type: |
|
| Period Type: |
|
|
| X |
- Details
| Name: |
us-gaap_StatementClassOfStockAxis=us-gaap_WarrantMember |
| Namespace Prefix: |
|
| Data Type: |
na |
| Balance Type: |
|
| Period Type: |
|
|
AEON Biopharma (AMEX:AEON)
Graphique Historique de l'Action
De Nov 2024 à Déc 2024

AEON Biopharma (AMEX:AEON)
Graphique Historique de l'Action
De Déc 2023 à Déc 2024
